The Laryngeal Mask Airway (LMA) is a cornerstone of modern anesthesia, representing one of the most significant advances in airway management since the endotracheal tube. Given its breadth, we will explore this topic across three detailed sections.
Section 1: The Laryngeal Mask Airway (LMA) - A Fundamental Revolution
Introduction: Bridging the Gap
Before the 1980s, airway management during anesthesia was largely a dichotomy: the face mask or the endotracheal tube (ETT). The face mask was simple but offered no airway protection and could be difficult to maintain a seal. The ETT provided a secure, protected airway but required laryngoscopy—a skill that can be difficult and is not without risk.
Enter the Laryngeal Mask Airway (LMA), invented by British anesthesiologist Dr. Archie Brain in 1981. His goal was to create a device that was less invasive than an ETT but more secure and reliable than a face mask. The LMA did exactly that, creating a "third option" in airway management and fundamentally changing anesthetic practice worldwide.
What is an LMA?
An LMA is a supraglottic airway device. This is a critical term: it means it sits above the glottis (the vocal cords and the opening to the trachea), unlike an ETT which sits within the trachea. It is composed of a wide-bore tube connected at one end to a standard 15mm connector (for the anesthesia circuit) and at the other end to an elliptical, inflatable cuff.
Mechanism of Action: The Perfect Seal
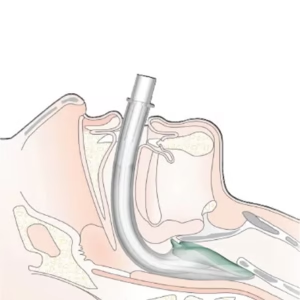
The genius of the LMA is its design. When the deflated cuff is inserted into the patient's mouth and advanced until it meets resistance, it sits in the hypopharynx. Upon inflation, the cuff molds to the contours of the laryngeal inlet, creating a low-pressure seal around the glottic opening.
This seal achieves two things simultaneously:
- It allows for effective positive-pressure ventilation: Gas from the anesthesia circuit is directed down the tube, through the mask, and into the trachea.
- It provides a degree of airway protection: While not as protective as an ETT's cuffed seal within the trachea, the LMA's seal prevents most secretions and regurgitated fluid from entering the glottis.
The device essentially acts as a "plug" that funnels air into the right place, all without the need for a laryngoscope or muscle relaxation.
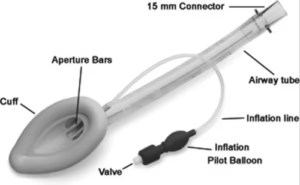
Anatomy of a Classic LMA
- Airway Tube (Shaft): The kink-resistant tube that connects the circuit to the cuff. It has a calibrated volume indicator to prevent over-inflation.
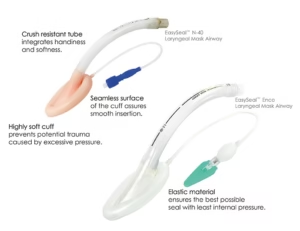
- Cuff (Mask): The inflatable, elliptical-shaped part made of medical-grade silicone or PVC. It is designed to fit the perilaryngeal anatomy.
- Pilot Balloon & Valve: A small balloon connected to the main cuff via a narrow channel. It allows the clinician to monitor the cuff's inflation pressure and to inflate/deflate it from a distance.
- 15mm Connector: The standard end-piece that connects to the breathing circuit, ventilator, or bag-valve mask.
The LMA's simplicity, ease of insertion, and hemodynamic stability (it doesn't trigger the same sympathetic response as laryngoscopy) made it an instant success. It is now a standard tool for millions of anesthetics globally.
In our next post, we will explore the vast array of LMAs available today, breaking them down into the two primary classification systems: Miller's functional groups and the evolutionary Generations.
Next: Classifying the LMA →
Page 1 of 3
Section 2: Classifying the LMA - From Miller's Groups to Modern Generations
The original LMA Classic was just the beginning. Today, a bewildering variety of supraglottic airway devices exists, each with subtle but important differences. To make sense of them, two main classification systems are used: the Miller Classification (based on reusability and function) and the Generational Classification (based on evolutionary design).
Classification Based on Miller (Functional Groups)
This system, proposed by Dr. David Miller, categorizes LMAs based on whether they are reusable or single-use, and whether they incorporate a channel for gastric access. This is a highly practical way to think about their capabilities.
| | | |
|---|
| Group 1 | Reusable LMA without a gastric access port. | The original design. For ventilation only. | LMA Classic™ |
| Group 2 | Reusable LMA with a gastric access port. | Allows passage of a gastric tube to drain stomach contents. | LMA ProSeal™ |
| Group 3 | Single-use (disposable) LMA without a gastric access port. | Cost-effective and eliminates infection risk. | LMA Unique™, Ambu AuraOnce™ |
| Group 4 | Single-use (disposable) LMA with a gastric access port. | Combines the safety of a gastric channel with the hygiene of a disposable device. | LMA Supreme™, Ambu AuraGain™ |
Classification Based on Generations
This system classifies LMAs by their evolution in design and function. It reflects the ongoing improvements in seal pressure, safety features, and versatility.
First Generation LMAs
These are the foundational devices. Their primary function is to serve as a conduit for ventilation.
- Design: A simple airway tube with a single-cuff mask.
- Function: Ventilation only.
- Limitations: Lower seal pressure (making them less suitable for positive-pressure ventilation or laparoscopic surgery), and no protection against gastric regurgitation.
- Examples:
- LMA Classic™: The original reusable device.
- LMA Unique™: The single-use version of the Classic.
- Ambu AuraOnce™: Another popular single-use first-generation device.
Second Generation LMAs
These devices were a major leap forward, designed specifically to address the limitations of the first generation, primarily the risk of aspiration.
- Design: Feature a gastric access channel (port) that runs parallel to the airway tube. They often have a modified cuff design (e.g., a dual-cuff or a dorsal cuff) to achieve a higher seal pressure in the pharynx.
- Function: Ventilation + Aspiration Protection. The gastric channel allows for the drainage of regurgitated fluid or the insertion of a gastric tube to decompress the stomach. The higher seal pressure allows for safer positive-pressure ventilation.
- Examples:
- LMA ProSeal™: The reusable pioneer of the second generation. Has a separate gastric outlet and a bite block.
- LMA Supreme™: A single-use, second-generation device with a built-in bite block and a rigid, anatomically curved tube that makes insertion easier.
- Ambu AuraGain™: A single-use device with a gastric channel and also features a channel to accommodate a flexible endoscope or a small-diameter endotracheal tube for intubation.
- i-gel™: A unique device in this class. It has a soft, gel-filled, non-inflatable cuff that conforms to the anatomy, and it includes a gastric channel.
Third Generation LMAs (Intubating LMAs)
This generation is defined by a specific new function: serving primarily as a dedicated conduit for blind or fiberoptic endotracheal intubation.
- Design: These are specially designed with a short, wide, rigid, and angled airway tube to facilitate the passage of an ETT.
- Function: Primarily for tracheal intubation. They are used in difficult airway scenarios where direct laryngoscopy has failed.
- Examples:
- LMA Fastrach™ (also known as the Intubating LMA or ILMA): The classic reusable intubating LMA. It comes with a dedicated set of silicone ETTs designed to pass through it easily.
- LMA CTrach™: An evolution of the Fastrach that incorporated built-in fiberoptic lenses and a screen, allowing the user to see the vocal cords during intubation. (Note: This device is no longer commercially available but was historically significant).
Understanding these classifications allows anesthesiologists to select the precise tool for the clinical scenario—whether it's a simple, short case, a patient at risk of aspiration, or a life-threatening difficult airway.
In our final section, we will cover the clinical application of the LMA: when to use it, when not to, how to insert it, and what complications can arise.
Next: Indications, Techniques, and Safety →
Page 2 of 3
Section 3: The LMA in Clinical Practice - Indications, Techniques, and Safety
The LMA is a remarkably versatile tool, but its safe and effective use depends on a clear understanding of its proper place in airway management. This post covers the practical aspects of using an LMA.
Indications: When is the LMA the Right Choice?
The LMA is an excellent choice in many clinical situations:
- Elective Surgery: For most routine procedures requiring general anesthesia where the patient is fasted and positioned supine (e.g., limb, breast, urological, ophthalmic surgery). It is ideal for short-to-medium duration cases.
- Airway Rescue: It is a core component of the Difficult Airway Algorithm. In a "Can't Intubate, Can Ventilate" (CICV) scenario, inserting an LMA can rapidly restore oxygenation and ventilation, buying critical time.
- Conduit for Intubation: As discussed, second and third-generation LMAs can be used to guide a fiberoptic bronchoscope or an endotracheal tube into the trachea in a patient with a difficult airway.
- Outpatient/Ambulatory Surgery: Its rapid emergence and low incidence of sore throat make it perfect for the fast-paced ambulatory setting.
- Emergency and Pre-Hospital Care: Its ease and speed of insertion make it valuable for paramedics and emergency physicians for managing an unconscious patient's airway.
Contraindications: When Should the LMA Be Avoided?
Knowing when not to use an LMA is as important as knowing when to use it.
Insertion Technique (Simplified)
- Preparation: Check the cuff for leaks by inflating it. Deflate it completely so it forms a smooth, flat spoon shape. Apply a water-based lubricant to the posterior surface.
- Patient Positioning: Place the patient in the "sniffing the morning air" position (neck flexed, head extended).
- Insertion:
- Open the patient's mouth widely.
- Press the deflated mask against the hard palate with the index finger.
- Using the index finger to guide it, slide the mask along the palate and down the posterior pharyngeal wall until you meet resistance. This is the "sweet spot."
- Remove the finger while holding the tube steady.
- Inflation: Inflate the cuff with the appropriate volume of air (e.g., 15-20 mL for a size 4). Do not over-inflate.
- Confirmation: Secure the LMA. Confirm correct placement by:
- Observing bilateral chest rise and fall.
- Seeing the reservoir bag move spontaneously with respiration.
- Listening for clear breath sounds over the lungs.
- Gold Standard: Observing a square-wave capnography tracing, which confirms exhaled CO2.
Potential Complications
While very safe, the LMA is not without risks.
- Common/Mild: Sore throat, dysphagia (difficulty swallowing), mild trauma to the lips, tongue, or uvula.
- Serious (but rare):
- Laryngospasm: A reflex closure of the vocal cords, often caused by stimulation during light anesthesia or removal.
- Pulmonary Aspiration: The most feared complication, though its incidence is low in fasted, elective patients.
- Nerve Injury: Temporary or permanent damage to the lingual, hypoglossal, or recurrent laryngeal nerves from pressure or malpositioning.
- Complete Airway Obstruction: If the device is malpositioned (e.g., the epiglottis is folded down).
Removal
The LMA can be removed either when the patient is deeply anesthetized or fully awake. Removing it while awake is generally preferred as it allows the patient to protect their own airway and reduces the risk of laryngospasm.
Conclusion
The Laryngeal Mask Airway transformed anesthesia by providing a safe, reliable, and minimally invasive alternative to the face mask and endotracheal tube. Its success lies in its elegant simplicity. However, like any tool, its mastery requires understanding its design, respecting its limitations, and applying it judiciously based on the patient and the procedure. From the first-generation Classic to the advanced second-generation devices, the LMA remains an indispensable part of the modern anesthesiologist's arsenal.
← Back to Introduction of LMA
Page 3 of 3